42Y/M C/o CKD 2* to Diabetic Nephropathy
This blog also reflects my patient centered online learning portfolio and valuable inputs on the comments box is welcome.
I have been given this case to solve in an attempts to understand the topic of patient clinical data analysis, to develop my competency in reading and comprehending clinical data including history, clinical finding, investigation
-------------------------------------------------------
A 42 year old male working as a rice farmer , hailing from Nalgonda presented to the OPD with shortness of breath , loss of consciousness 2 days ago
history of Present illness
patient was apparently asymptomatic 15 years ago
15 years ago , he had complaints of polyuria , nocturia , polyphagia , polydispsia and dizziness , he went to a government hospital and he was diagnosed with DM 2 , he reported that he is taking the prescribed medication regularly .
5 years ago he had dragging type of pain at the back of head , he went to a local hospital where he was diagnosed with HTN , pateint reports taking the prescribed medication regularly
1 year ago he complained of shortness of breath , pedal edema , weakness and dizziness after visiting a government hospital after a fainting spell , he had a creatinine level of 7 and was recommended to start dialysis
the patient has been on dialysis for 1 year , 2 months ago he reported paroxysmal nocturnal dyspnoea
2 days ago , during his routine dialysis , he had 3 episodes of vomiting and shortness of breath and was intubated
history of past illness
he is a known case of DM2 , HTN
he is n/k/c/o epilepsy , asthma , tuberculosis
personal history
diet : mixed
appetite : normal
occupation : rice farmer
micturition : on a foleys catheter
bowel movements : reduced
addictions : reports intake of alcohol occasionally
smoked cigarettes occasionally
allergies : not known
family history
- elder brother and younger sister have DM 2
---------------------------------------------------------------------------
examination
general examination
pallor : present
icterus : absent
cyanosis : absent
clubbing : absent
lymphadenopathy : absent
pedal edema : present , pitting type pedal edema , reduces on rest and elevation


vitals :
pulse rate : 74bpm
rr : 22cpm
BP : 150/100 mmHg
systemic examination
CVS
-thrills : no
- cardiac sounds : S1 S2 heard
-cardiac murmurs : no
Respiratory system
position of trachea : central
dyspnoea : present
wheeze : no
PA
normal
CNS
normal
on examination of nails
he has onychomycosis


INVESTIGATIONS




provisional diagnosis
chronic kidney disease secondary to Diabetic nephropathy
Case update 1/07/2022
Today nephrology update
Icu bed 4
http://drkulkarnimd.blogspot.com/2022/06/42m-with-sudden-sob-and-pedal-edema.html
Day 1 :
S - patient is off sedation & paralysis and moving all 4 Limbs and responding to commands (1 step )
O - bp 140/90
Pr 82 cpm
RR 22 cpm
Spo2 97%
Cvs S1 S2 heard
RS - BAE PRESENT
E4VtM6



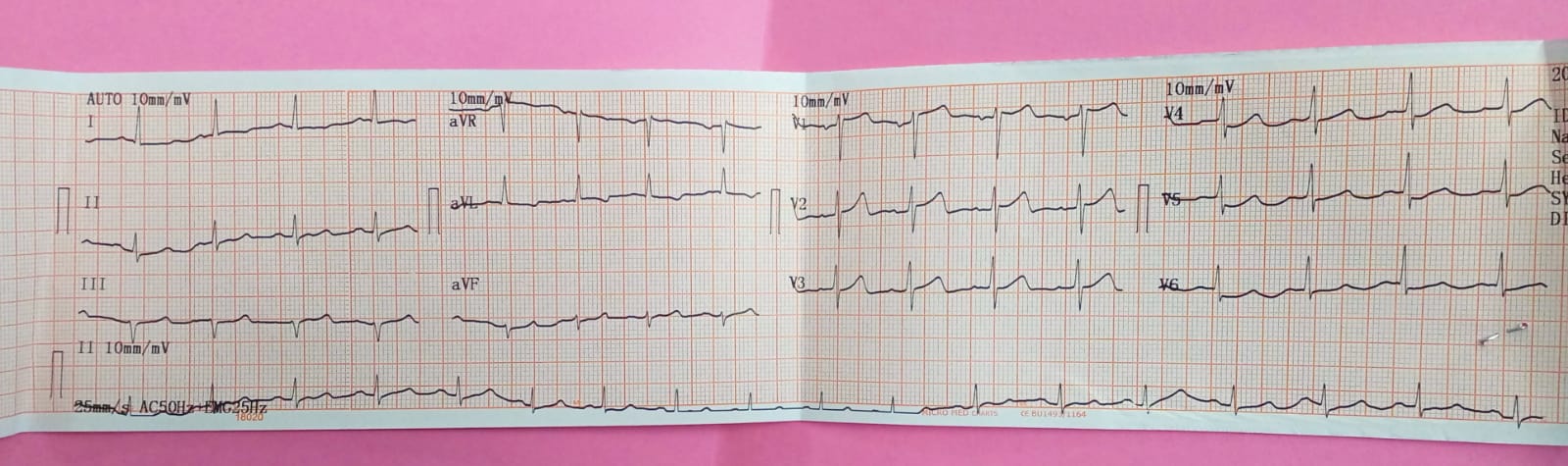
A - acute cardiogenic pulmonary edema 2to ?NSTEMI with ? Aspiration pneumonia
P - plan to extubate if criteria meets.
Case update : 2/07/2022
- The patient has been extubated and his ryles tube is scheduled to be removed today
Icu bed 4
http://drkulkarnimd.blogspot.com/2022/06/42m-with-sudden-sob-and-pedal-edema.html
Day 4 :
S - patient is off sedation & paralysis and moving all 4 Limbs and responding to commands
On Over night T piece
Yesterday HD was taken
O - bp 130/90
Pr 82 cpm
RR 22 cpm
Spo2 97%
Cvs S1 S2 heard
RS - BAE PRESENT
E4VtM6
A - acute cardiogenic pulmonary edema 2to ?NSTEMI with ? Aspiration pneumonia with CRF secondary to ?Diabetic nephropathy ?Nsaid induced nephropathy
P - plan to extubate as criteria met for extubation.

Comments
Post a Comment