Nephrology case
This is an online e log book to discuss our patient identified health data shared after taking his/her guardian signed informed consent. Here we discuss our individual patient problems through a series of inputs from available global online community of experts with a aim to solve those patients clinical problem with collective current best evidence based inputs.
This blog also reflects my patient centered online learning portfolio and valuable inputs on the comments box is welcome.
I have been given this case to solve in an attempts to understand the topic of patient clinical data analysis, to develop my competency in reading and comprehending clinical data including history, clinical finding, investigation.
A 32 year old man had come to the OPD with complaints of pedal edema , low urine output and shortness of breath since the past 4 days
he is a known case of hypertension since the past one year and is on medicationThe patient used to work as an autodriver and his daily routine consisted of him waking up at 6am and he drove children to school , his average work day ended at 8pm after which he used to have an occational drink with his friends . During the first lockdown the patient had headcahe , dizziness and blurring of vision for which he had gone to a hospital in nalgonda and there he was diagnosed with hypertension with retinopathy and was started on Telma.H and was referred to another hospital where he had gotten a creatinine test done and the level was 8.6 and we has started on Arkamin tablets this was done 7 months ago .
due to the prognosis of his CKD he was referred to KIMS for dialysis and had been getting dialysis done since the past 8 months , he developed backpain and headache 4 months ago and had pitting type pedal edema both of these issues were relieved when the patient rested for a while .
cheif complaints
-decreased urine output
-pedal edema
-shortness of breath
History of present illness
-patient developed dizziness and blurring of vision 1 year ago
-he was diagnosed with hypertension associated retinoapathy and was started on Tab. telma.h since the past year
-he developed backpain 4 months ago and pedal edema pitting type 1 month ago
-on 18th September the patient was referred to the orthopedic department , there was tenderness at the L4 ,L5 region
no neurologial deficiets noted
-on 19th september ; the patient was diagnosed with CKD on MHD , hypertensive retinopathy
History of past illness
-a known case of Hypertesion since 1 year
-n/k/c/o DM,thyroid,TB
Personal history
-occupation : auto driver
-diet :mixed
-appetite : normal
-bowels : regular
-micturition :decreased urine output
-no known allergies and no addictions
-occasionally consumes 180ml of Alcohol at social gatherings
Family history
-his elder brother id a known case of hypertension since 16 years
General Examination
-patient was conscious , coherent and coherent and examined in a well lit room
VITALS
-pulse rate : 99bpm
-respiratory rate : 19/min
-BP: 150/80 mmHg
-Temperature : Afebrile
-GRBS : 127mg%
-SpO2: 98% at room temperature
physical examination
-pallor : not present
-icterus : not present
-cyanosis : not present
-clubbing : not present
-lymphadenopathy : not present
-generalised anasarca is seen
-pedal edema : present , pitting type
-malnutrition is absent
Systemic examination
-cardiovascualr system
~S1 and S2 are heard
-no thrills and no murmurs
-Respiratory system R
~vesicular breath sounds heard
-trachea is in central position
-no wheezing
-no dyspnoea
on 7th october the patients Oxygen saturation was dropping and reached 40% , so since then the patient has been given humidified oxygen
- on 8th october JVP was seen prominently and Rhonchi was heard , the patient was put on nebulization with budecort vials
-Abdomen
~obese shaped abdomen
-no tenderness
-no palpable mass
-no hernial orifices
-no free fluid
-liver and spleen are not palpable
-bowel sounds are heard
-CNS
~Conscious and normal speech
-normal gait
-crainal nerves are normal
-sensory system is normal
-motor system is normal
Reflexes
right left
biceps +2 +2
triceps +2 +2
supinator +2 +2
knee +2 +2
ankle +2 +2
INVESTIGATIONS
On 2nd September
Ultrasound report

On 4th September
Ultrasound report

grade 2 fatty liver is present

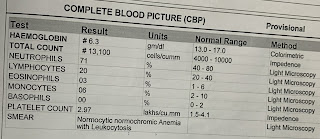
hemoglobin is 6.3 which is below normal
WBC count is 13,100 which is above normal
On 5th September




On 29th September


urea is 89mg/dl which is above normal
creatinine is 10.2 mg/dl (above normal)
chloride is 96mEq/l which is below normal
On 5th October





Color Doppler

Patient images
-generalised edema and pitting edema




on 6th october




CKD on MHD secondary to Hypertensive nephropathy
PLAN OF MANAGEMENT:
Renal Transplantion
TREATMENT :
On 5/10/21 :
Fluid restriction <1L/day
Salt restriction <2.4L/day
T.Lasix 40mg PO/BD
T.Nicardia 20mg PO/TID
T.Arkamine 0.1 mg PO/BD
T.Shelcal CT po/od
T.Nodosis 500 mg
T.Met XL 50 mg po/od
INJ erythropoietin 4000 units weekly once
BP monitering
On 6/10/21 :
Fluid restriction <1L/day
Salt restriction <2.4L/day
T.Lasix 40mg PO/BD
T.Nicardia 20mg PO/TID
T.Arkamine 0.1 mg PO/BD
T.Shelcal CT po/od
T.Nodosis 500 mg
T.Met XL 50 mg po/od
INJ erythropoietin 4000 units weekly once
BP monitering
On 7/10/21
Fluid restriction <1L/day
Salt restriction <2.4L/day
T.Lasix 40mg PO/BD
T.Nicardia 20mg PO/TID
T.Arkamine 0.1 mg PO/BD
T.Shelcal CT po/od
T.Nodosis 500 mg
T.Met XL 50 mg po/od
T.Metolazol 5 mg po/ bd
INJ iron sucrose 100 mg iv / bd
INJ erythropoietin 4000 units weekly once
Update : 11th October



This elog was done with the help of Dr. Surya (intern ) http://saisurya100.blogspot.com/2021/10/32-yr-old-man-with-ckd-on-mhd-with.html
I sincerely thank Dr.Rakesh and Dr.Surya for providing this learning opportunity .

Comments
Post a Comment